



Obsessive-compulsive disorder (OCD) is not classified as an anxiety disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). While OCD often involves intense anxiety and commonly co-occurs with anxiety disorders, it is now placed in its own category: Obsessive-Compulsive and Related Disorders.
About 1.2% of U.S. adults experience OCD each year, and 2.3% will experience it at some point in their lives, underscoring the importance of accurate classification and treatment.
What is OCD?
Obsessive-compulsive disorder (OCD) is a mental health condition marked by two core symptoms:
- Obsessions: Unwanted, intrusive thoughts, images, urges, or sensations that cause intense anxiety or distress.
- Compulsions: Repetitive behaviors or mental rituals performed to reduce the anxiety or prevent something feared from happening.
This cycle of obsessions and compulsions can be time-consuming, emotionally draining, and disruptive to daily life.
Why OCD was reclassified
Although anxiety is a major part of OCD, the disorder is no longer classified as an anxiety disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). In 2013, OCD was moved to a new category: Obsessive-Compulsive and Related Disorders, which also includes:
- Body dysmorphic disorder (BDD)
- Hoarding disorder
- Trichotillomania (hair-pulling disorder)
- Excoriation (skin-picking disorder)
This reclassification reflects the unique features of OCD, especially the repetitive, ritualistic behaviors and the specific nature of intrusive thoughts.
“Every person with OCD experiences anxiety,” says Tracie Ibrahim, LMFT, CST, Chief Compliance Officer at NOCD. “No one with OCD has ever escaped the feeling of anxiety—that’s the whole problem—that you feel so anxious that you engage in compulsions to try to get rid of the discomfort.”
How are OCD and anxiety disorders related?
While OCD is not classified as an anxiety disorder, it is closely linked to anxiety.
- Anxiety is a core feature of OCD: Obsessions (intrusive, distressing thoughts) trigger anxiety and compulsions are performed in an attempt to temporarily relieve that anxiety.
- High comorbidity rates: Research shows that many people with OCD also meet criteria for at least one anxiety disorder. For example, a study of children and adolescents found that nearly half of those with OCD also had another anxiety disorder.
- Shared symptoms: Excessive worry, restlessness, and physical tension may appear in both OCD and generalized anxiety disorder (GAD).
The key distinction is in what drives the anxiety. In OCD, anxiety is triggered by intrusive thoughts and maintained by compulsions, whereas in anxiety disorders, worry tends to be more general, persistent, and tied to real-life situations rather than specific obsessions.
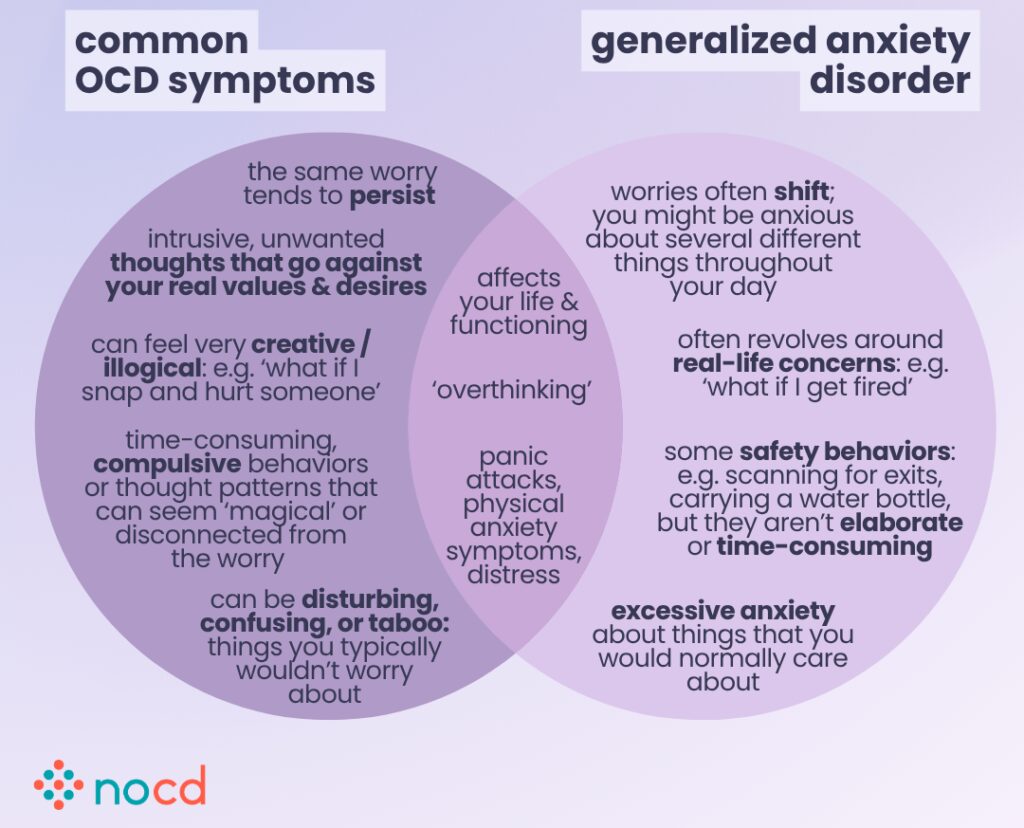
Key differences: OCD vs. anxiety disorders
OCD differs from other anxiety disorders–like generalized anxiety disorder (GAD), panic disorder, or social anxiety–in several important ways:
1. OCD follows a specific pattern
OCD typically follows a structured cycle: intrusive thought (obsession) → intense anxiety → compulsion to neutralize the fear → temporary relief.
In contrast, anxiety disorders usually involve persistent worry or fear that does not induce ritualistic behaviors.
2. Compulsions are central to OCD
People with OCD perform rituals or mental acts (e.g., checking, cleaning, reassurance-seeking) in response to their obsessions.
In most anxiety disorders, behaviors are generally reactive, not ritualistic.
“There’s only one thing that makes OCD and anxiety different, and that’s obsessions and compulsions,” says Ibrahim.
3. OCD themes are more specific and repetitive
OCD often fixates on themes such as:
- Contamination (e.g., fear of germs or illness)
- Harm
- Morality
- Order
- Symmetry
Anxiety disorders may involve similar fears, but they usually focus on real-life situations and are less repetitive or irrational.
Comparison chart: OCD vs. anxiety disorders
Below is a quick comparison chart to help clarify:
| OCD | Anxiety disorders |
| Unwanted, intrusive thoughts (obsessions) | Excessive worry, fear, or dread about future events or social situations |
| Compulsive behaviors or mental rituals to neutralize anxiety | Reactive behaviors, no compulsions |
| Repetitive cycle: obsession → anxiety → compulsion → temporary relief | Persistent worry tied to real-life situations |
| Specific and repetitive, e.g., contamination, morality, or harm | Usually situation-based, less repetitive or irrational |
Can you have OCD and an anxiety disorder?
Yes. It’s common to have both OCD and an anxiety disorder. Research suggests that around one-third of people with OCD also meet criteria for a co-occurring anxiety condition, such as:
- Generalized anxiety disorder (GAD)
- Social anxiety disorder (SAD)
- Specific phobias
Having both conditions can intensify symptoms and make treatment more challenging, as each condition can reinforce the other.
Treatment for OCD and anxiety disorders
Effective treatment is available for both OCD and anxiety disorders, though approaches must be tailored to the specific condition.
OCD treatment: exposure and response prevention (ERP) therapy
The most effective treatment for OCD is exposure and response prevention (ERP) therapy, a type of cognitive behavioral therapy (CBT). Unlike standard CBT, ERP specifically targets the obsession-compulsion cycle, helping individuals face anxiety-provoking thoughts without performing compulsions.
“ERP helps people tolerate discomfort and teaches them that they don’t need to perform compulsions to feel safe,” says Ibrahim.
Research shows that ERP is highly effective, with 80% of people experiencing significant symptom reduction.
Other approaches that may help include:
- Medication (typically SSRIs)
- Mindfulness-based strategies
- Acceptance and commitment therapy (ACT)
These are typically done in combination with ERP therapy, depending on the individual’s needs.
Severe or treatment-resistant OCD may benefit from the following therapies:
- Intensive outpatient programs (IOPs)
- Partial hospital programs (PHPs)
- Residential treatment centers (RTCs)
- Transcranial magnetic stimulation (TMS)
- Deep brain stimulation (DBS)
- Gamma knife radiosurgery (GKRS)
Anxiety disorder treatment
- Standard CBT
- Medication (like SSRIs)
- ERP therapy (particularly when intrusive thoughts play a major role)

Find the right OCD therapist for you
All our therapists are licensed and trained in exposure and response prevention therapy (ERP), the gold standard treatment for OCD.
Bottom line
OCD and anxiety disorders can share symptoms, but they are distinct conditions. The hallmark of OCD is the presence of obsessions and compulsions. Recognizing this distinction is crucial for accurate diagnosis and effective, evidence-based treatment.
Key takeaways
- OCD is not classified as an anxiety disorder, despite anxiety being a core feature.
- The defining traits of OCD are intrusive thoughts (obsessions) and compulsive behaviors.
- Anxiety disorders often involve worry and fear, but not ritualistic compulsions.
- Many people experience both OCD and an anxiety disorder, and both are treatable.
- Exposure and Response Prevention (ERP) therapy is a highly effective treatment for OCD and anxiety disorders.
